
If you have ever looked at an IHSS Notice of Action and wondered how the county actually decided on the number of authorized hours, you are not alone. One of the most misunderstood parts of California’s In-Home Supportive Services program is the Functional Index Ranking system and the Hourly Task Guidelines counties use during assessments. Families often assume IHSS hours are based mostly on diagnosis or medical severity. In reality, the system is supposed to focus on something much more specific: functional limitations. And, quite honestly, that distinction matters enormously.
Two children with the exact same diagnosis may receive completely different hour totals depending on how their daily functioning presents in real life. One child with autism may independently toilet, dress, and stay safe with minimal prompting. Another child with autism may require constant redirection, hands-on assistance, sensory regulation, supervision around danger, and extensive support throughout nearly every activity of daily living.
IHSS is not designed to measure diagnoses alone. It is supposed to measure how much human assistance is actually required for a person to safely function day to day.
Understanding how Functional Index Rankings and Hourly Task Guidelines work can help families prepare for assessments, understand Notices of Action, identify missing hours, and better advocate for services that accurately reflect the true level of caregiving occurring inside the home.
What Are Functional Index Rankings?
Functional Index Rankings are the scoring system IHSS social workers use to assess how much assistance a recipient needs in specific daily living activities. These rankings are assigned separately across multiple service categories and are used alongside statewide Hourly Task Guidelines to calculate authorized service hours.
These rankings come directly from California regulations under Title 22 and are intended to standardize assessments statewide while still allowing room for individualized circumstances.
The rankings generally fall on a scale from 1 through 5:
A ranking of “1” means the recipient is independent and can safely perform the activity without human assistance.
A “2” means the recipient can perform the activity but needs verbal assistance such as reminders, guidance, prompting, or encouragement.
A “3” means the recipient can perform part of the activity but requires some direct physical human assistance.
A “4” means the recipient can perform only a small part of the activity and requires substantial human assistance most of the time.
A “5” means the recipient cannot perform the activity at all and is completely dependent on another person.
While these definitions sound simple on paper, their real-world application becomes far more nuanced during actual assessments.

The Most Important Thing Families Miss: Function vs. Capability
One of the biggest misunderstandings in IHSS is the difference between being physically capable of doing something versus being functionally able to complete it safely and consistently. This distinction changes everything so it’s important to understand.
For example, a child may technically be able to hold a toothbrush and move it around their mouth. But if that child cannot sequence the task, requires repeated prompting, becomes behaviorally dysregulated, attempts to flee the bathroom, forgets major steps, or cannot safely complete the activity without intervention, that child may not truly be independent in that activity from an IHSS standpoint.
The same applies across nearly every category.
A child who can physically walk may still require extensive assistance with mobility if they wander unsafely, fall frequently, lack danger awareness, or require constant physical guidance. A teenager who can physically feed themselves may still require hands-on support if behavioral issues, impulsivity, or cognitive impairments interfere with safe eating.
IHSS assessments are supposed to evaluate real-world functioning — not isolated physical ability observed during a short home visit.
Rankings Are Assigned Separately for Each Task
Many families mistakenly believe IHSS assigns one overall “severity score,” but that is not how the system works. Each service category receives its own separate ranking.
For example, a recipient might receive:
- A “5” in toileting
- A “4” in bathing
- A “3” in dressing
- A “2” in feeding
- A “1” in respiration
These rankings are then combined with the Hourly Task Guidelines to calculate monthly authorized time for each category.
The specific categories often assessed include:
- Bathing, oral hygiene, and grooming
- Dressing
- Feeding
- Bowel and bladder care
- Menstruation care
- Repositioning
- Ambulation and Transfers
- Respiration assistance
- Memory, orientation, and judgment (for Protective Supervision)
- Domestic services
- Related services
Each category is evaluated independently because a person’s functioning may vary dramatically across activities.
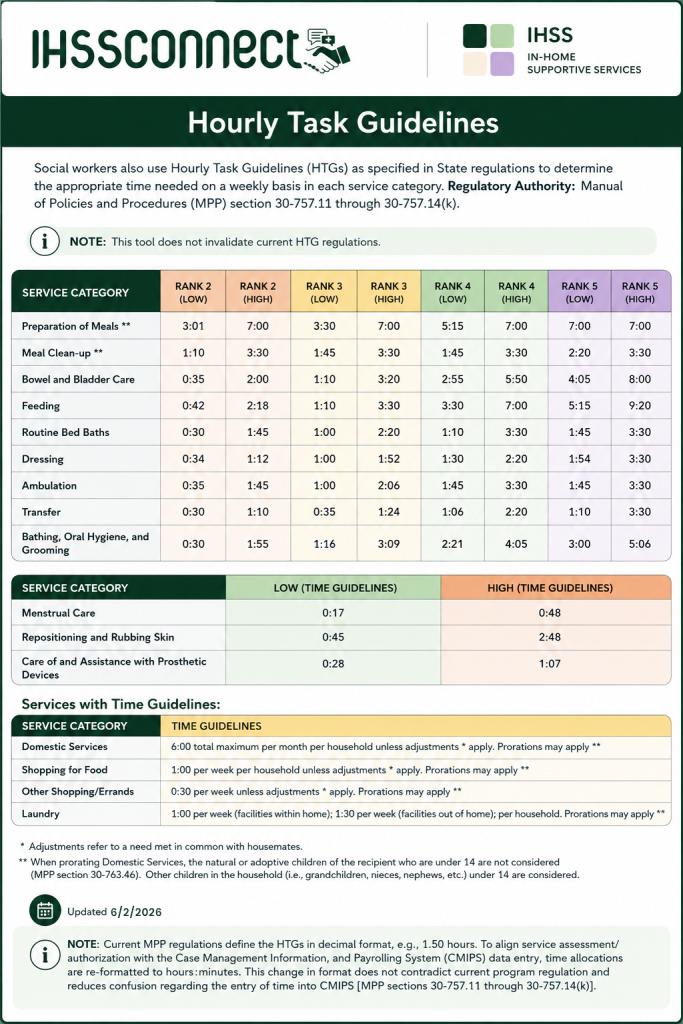
What Are the Hourly Task Guidelines?
Once rankings are assigned, counties apply statewide Hourly Task Guidelines. These are estimated ranges of time associated with different service categories and ranking levels.
The Hourly Task Guidelines are not supposed to function as rigid caps or automatic formulas. They are intended to provide a framework while still allowing counties to account for individualized needs and extraordinary circumstances. Key word being extraordinary.
Unfortunately, many families experience assessments where guidelines are treated more like hard ceilings rather than flexible tools. You should know that is not how the regulations were intended to work.
For example, a child with significant sensory dysregulation, severe behavioral challenges, seizure risks, or major mobility impairments may reasonably require substantially more time for bathing or dressing than the “average” recipient contemplated within the standard task ranges.
If a recipient’s disability-related needs significantly extend the amount of time required to safely complete a task, those details should be specifically documented and explained.
Human Assistance vs. Verbal Assistance
One of the more important distinctions in Functional Index Rankings is the difference between verbal assistance and human assistance.
Verbal assistance generally refers to cueing, reminding, encouraging, redirecting, or guiding someone through a task without physically helping them perform it.
Human assistance means actual physical involvement.
This distinction can dramatically impact rankings and ultimately authorized hours.
For example:
- A child who only needs reminders to brush their teeth may receive a “2.”
- A child who requires hand-over-hand assistance to complete brushing may receive a higher ranking.
- A child who actively resists care, requires behavioral intervention, or cannot physically complete the task safely alone often requires a ranking in the “4” or “5” range depending on need.
The details matter enormously.
This is why vague statements like “needs help” are often less effective during assessments than highly specific descriptions of what caregiving actually looks like. If physical assistance is required for any activity or task, make sure that is properly communicated to the social worker—and properly documented in the the recipient’s various forms.

Children Are Compared to Same-Age Peers
This is one of the most important concepts in pediatric IHSS cases.
Children are not assessed in a vacuum. Counties compare a child’s functioning against what would normally be expected of a non-disabled child of the same age.
That means some level of caregiving may be considered age appropriate and therefore not compensable under IHSS.
For example, most toddlers naturally require help with dressing, bathing, and supervision. But if a teenager requires the same level of assistance, that may strongly support higher rankings and additional service hours.
This “same-age peer” comparison becomes critically important in cases involving developmental disabilities, autism, intellectual disabilities, traumatic brain injuries, and cognitive impairments.
Parents sometimes unintentionally minimize their child’s needs because they have become accustomed to providing extraordinary levels of care every day. But the county is supposed to evaluate whether those needs exceed what would normally be expected for a child of similar age without disabilities.
Why Cognitive Impairments Matter So Much
Another area where families often encounter problems is when counties focus too heavily on physical ability while overlooking cognitive limitations.
A person may physically be able to walk, feed themselves, or complete certain motions, but cognitive impairments may still create significant functional limitations.
This is especially true in cases involving:
- Autism
- Intellectual disability
- Traumatic brain injury
- Dementia
- Severe ADHD
- Neurological disorders
- Mental impairments affecting judgment or sequencing
A recipient who lacks awareness of danger, cannot remain on task, forgets steps, wanders, impulsively engages in unsafe behaviors, or cannot complete activities consistently may still require substantial assistance even when physical strength exists.
That is why documentation from IEPs, IPPs, neuropsychological evaluations, behavioral reports, occupational therapy assessments, and physician records can become extremely important during IHSS assessments.
Protective Supervision Is Different
Protective Supervision operates differently than task-based services.
Instead of focusing primarily on physical assistance with activities of daily living, Protective Supervision addresses the need for 24-hour monitoring due to dangerous behaviors caused by mental impairment, cognitive limitations, or poor judgment.
Families are sometimes incorrectly told their child “already receives enough hours” through task-based services, as though Protective Supervision simply overlaps with those categories. It does not.
Protective Supervision exists because some recipients cannot safely remain alone due to:
- Wandering or elopement
- Self-injury
- Aggression
- Ingestion risks
- Unsafe impulsive behaviors
- Inability to recognize danger
- Severe judgment impairments
- Dangerous sensory-seeking behaviors
A recipient can qualify for substantial task-based hours and still separately qualify for Protective Supervision.
What Social Workers Are Actually Evaluating
During assessments, social workers are often evaluating much more than families realize.
They may be observing:
- Ability to initiate tasks
- Ability to sequence steps
- Safety awareness
- Consistency of functioning
- Physical participation
- Endurance and fatigue
- Behavioral interference
- Need for prompting
- Need for redirection
- Ability to complete tasks
- Cognitive understanding
- Risk factors during activities
This is why brief observations during calm moments can sometimes create inaccurate impressions.
A child who appears calm and cooperative during a one-hour home visit may behave very differently during stressful routines like bathing, toileting, transitions, sensory overload, bedtime, or community outings.
Families should not assume the county automatically understands those realities unless they are clearly explained and documented. If you or someone you know is struggling in this process and need help with an appeal, consider using an IHSS advocate.
Documentation Is Everything
The strongest IHSS cases usually show consistency across multiple records.
The county assessment should align with:
- IEPs
- IPPs
- Behavioral reports
- Therapy notes
- Medical records
- Caregiver logs
- Incident reports
- Neuropsychological evaluations
- School observations
Specific functional descriptions are usually much stronger than general statements.
For example:
“He attempts to leave the home several times daily without understanding environmental dangers.”
“She requires hand-over-hand assistance throughout toileting and hygiene routines.”
“He lacks safety awareness around hot surfaces and traffic and requires continuous intervention.”
“She becomes behaviorally dysregulated during bathing and requires two-person assistance to safely complete hygiene tasks.”
Concrete examples paint a much clearer picture than diagnosis labels alone.
Counties Do Not Always Get It Right
IHSS assessments are conducted by human beings, and human beings make mistakes.
Some social workers are highly experienced and thorough. Others may misunderstand disabilities, rely too heavily on brief observations, incorrectly apply hourly guidelines, overlook cognitive impairments, or fail to fully account for extraordinary caregiving demands.
That is why families who understand the Functional Index Ranking system are often better equipped to identify missing hours, inaccurate rankings, or overlooked service categories.
Understanding the framework does not guarantee approval, but it does allow families to advocate more effectively and recognize when authorized hours may not reflect the true level of care being provided.
The IHSS Functional Index Rankings and Hourly Task Guidelines form the backbone of how California determines authorized caregiving hours. But the process is far more individualized than many families realize.
The system is supposed to evaluate how a person actually functions in daily life — not simply what diagnosis appears on paper.
Families should never assume the county automatically understands the full extent of caregiving occurring inside the home. What has become “normal” to you may actually represent extraordinary levels of daily support compared to a same-age peer without disabilities.
Understanding how rankings work, how task guidelines are applied, and how functional limitations are evaluated can help families prepare for assessments, strengthen documentation, and better advocate for services that accurately reflect real-world caregiving needs.
And when families need to find caregivers who already understand the realities of IHSS, Protective Supervision, cognitive impairments, mobility limitations, and complex home care, platforms like IHSS Connect are helping families and providers connect across California through a free, purpose-built registry designed specifically for the IHSS community.


